 John McCain has served in the Senate since 1987. He occupies the seat that used to belong to Barry Goldwater (a conservative who lost in a landslide in the Presidential election in 1964; Senator Goldwater would eventually repudiate a number of his ultra conservative policy stances from earlier in his life). Senator McCain is 81 years old and has been getting treatment for brain cancer that was publicly announced in the summer of 2017. This piece is an appreciation for his service to the United States in both the Navy and Congress. A recent dual biography on the Bush Presidents is titled The Last Republicans, but that label fits Senator McCain much better (that said, even the latest Star Wars title shows that the “last anything” is probably hyperbole, except in cases like this or this).
John McCain has served in the Senate since 1987. He occupies the seat that used to belong to Barry Goldwater (a conservative who lost in a landslide in the Presidential election in 1964; Senator Goldwater would eventually repudiate a number of his ultra conservative policy stances from earlier in his life). Senator McCain is 81 years old and has been getting treatment for brain cancer that was publicly announced in the summer of 2017. This piece is an appreciation for his service to the United States in both the Navy and Congress. A recent dual biography on the Bush Presidents is titled The Last Republicans, but that label fits Senator McCain much better (that said, even the latest Star Wars title shows that the “last anything” is probably hyperbole, except in cases like this or this).
John McCain was born in 1936. His father and grandfather were both four-star admirals in the Navy. Mr. McCain graduated from the Naval Academy in 1958 and became an aviator. He was shot down over Hanoi in October of 1967. His ejection from the plane broke both arms and his right leg. Those breaks were not properly set. During his captivity, he was tortured by the North Vietnamese, causing further injuries. Because of his family connections, he was offered an opportunity to be repatriated (swapped for other prisoners) before other Americans that were captured. Mr. McCain always refused such offers. His captors tried to break him, hanging him by his broken arms for hours (you can read about it in Robert Timberg’s The Nightingale’s Song). He was finally released in 1973. He was elected to the House of Representatives in 1982 and served two terms before successfully running for Senate.
In his masterful book on the 1996 Presidential Primaries and Election, The Losers, Michael Lewis met and fell for John McCain (to be clear, Lewis identifies as a liberal but deeply liked and admired the Senator anyway). The Senator was not running for President, but was serving as a surrogate for Senator Bob Dole. While Mr. McCain was imprisoned in the Hanoi Hilton, American anti-war protest speeches were broadcast into the prison cells in an effort to break the men. The leader of one of the protests was David Ifshin. In a story that wasn’t known until the Clinton Administration, Mr. Ifshin apologized to Senator McCain in 1986. During the 1992 campaign, Mr. Ifshin served as a legal counsel to Governor Clinton but did not immediately work in the administration. When Senator McCain learned that his Vietnam protests were holding up an appointment, he called an unprompted press conference to help Mr. Ifshin. Here is another telling passage by Mr. Lewis:
I visited him at his home in Phoenix and at his cabin in the Arizona desert. I came to know his wife and children. But — and here was the amazing thing — simply by being weirdly insistent on hanging around I came across all sorts of little habits he had that said something about who the man was. McCain was clearly ambitious as they come; even then you could see he was talking himself into running for president. Yet he had developed a trick to ward off the ill-effects of ambition on his soul: he did many things that were of no possible benefit to his political career. For instance, he made a habit, once a week, at the crack of dawn, of visiting the hospital bed of retired Arizona congressman Mo Udall. Udall, who was dying of Parkinson’s disease, was unaware he had a visitor. When he’d been in power everyone wanted to see him; now no one but McCain came to visit. There was no one to witness McCain’s gesture. The visit was McCain’s way of paying tribute to a man he had admired, and who had guided him early in his career. Since Udall no longer responded to visitors, the visits were of no possible benefit to him. McCain did it for himself: the trips were a tool for reminding himself of the transience of political success. (304)
Senator McCain would run for President in 2000, but he was defeated by Governor Bush in the Republican primary. Senator McCain had upset Governor Bush by 19 points in New Hampshire and had momentum heading into the South Carolina primary. Karl Rove convinced George W. Bush to “take the gloves off” and Mr. Rove engineered a series of false and disgusting attacks that would ultimately help Bush win South Carolina and the nomination. One was that his wife Cindy was a drug addict (she had abused pain killers after a surgery in 1994). Another was that McCain had slept with prostitutes and given his wife STDs. Yet another was that he was turned in the Hanoi Hilton and was now mentally ill. The coup de grace was that he had a Negro child out of wedlock. This played into the racism that strongly existed (and still exists) in South Carolina and was a twisted distortion of a wonderful story: the McCains adopted a Bangladeshi orphan with a cleft palet named Bridget in 1991 after Cindy McCain met her during a relief mission. I am extremely proud that I voted for Senator McCain in the 2000 Republican primary.
Senator McCain championed campaign-finance reform and worked across the aisle with Russ Feingold in 2002. During the next few years, he rebelled less against the Republican establishment and sometimes went against earlier positions. He did this in an effort to shore up his base to run for President in 2008. His running mate was Sarah Palin, an unmitigated disaster that he thrust upon the nation when his advisors discouraged him from naming Senator Lieberman (a conservative Democrat) as his running mate. Senator McCain has never spoken poorly of her in public, but Steve Schmidt, his campaign manager, has voiced both his opinion on Governor Palin and where the GOP has been headed in recent years. In the general election that year, I voted for the other guy. Over the next few years, Mr. McCain would return to his maverick ways.
Fast forward to June of 2015. Donald Trump said this about Senator McCain, “He’s not a war hero. He was a war hero because he was captured. I like people who weren’t captured.” In previous elections, such a statement about a decorated veteran would have been disqualifying. More so than anything else in 2015, that moment was the one that signaled shift in the Republican party and its voters. Numerous people that claim to support the military have twisted themselves with irrational verbal gymnastics in order to justify Mr. Trump’s anti-veteran statement about Senator McCain.
J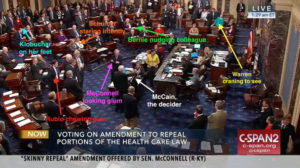 ust after his cancer diagnosis and treatment, the Republicans attempted to repeal the Affordable Care Act. Senator McCain ripped the Republicans for their terrible legislative process (no hearings, fast votes) and flew back to Washington to cast his vote. You can read about it here, but this video and picture say it all.
ust after his cancer diagnosis and treatment, the Republicans attempted to repeal the Affordable Care Act. Senator McCain ripped the Republicans for their terrible legislative process (no hearings, fast votes) and flew back to Washington to cast his vote. You can read about it here, but this video and picture say it all.
This December, there have been a number of moving moments and tributes. Vice President Biden appeared on The View, co-hosted by Meghan McCain. He was discussing his book about his son Beau, who passed away in 2015 from a similar form of brain cancer. Ms. McCain understandably was teary, and Mr. Biden moved over to console her. He said, “One of the things that gave Beau courage, my word, was John. You may remember when you were a little kid, your dad took care of my Beau. And Beau talked about your dad’s courage — not about illness, but about his courage.”
If you pay attention, you’ll see this over and over again in regards to Senator McCain. Political opponents having gracious and moving words to say on his behalf. Regardless of their fields, anyone who can garner such respect out of so many opponents is truly a special individual.
A few days later, Fred Hiatt, the Editorial Page Editor of the Washington Post wrote an opinion piece on Senator McCain and his role in U.S. global leadership, something that is very much lacking in the present:
Like many people, I’ve been alternately cheered and disappointed by McCain’s stances on domestic matters over the years — admiring when he helped save Obamacare a few months ago, disappointed when he went along with the Republican tax-cut bill this month. But McCain has never wavered in his support for democracy and human rights, and in his conviction that the United States needs to provide moral support to those who fight for freedom around the world. With President Trump often expressing more admiration for dictators than for democratic leaders, McCain’s advocacy has become lonelier — and more essential.
But he does not disguise how worried he is by the deeper currents that recall to him the darker movements of the 1930s: the nativism, the assaults on freedom of the press and the rule of law, the blaming of foreign competition for all ills, the rise of extremism. “I worry about the polarization that’s going on here, I really do,” McCain said. “The terms of the debate is what is really disappointing. The other day I was flipping the channels, and I saw Bannon just beating the crap out of Romney,” he continued, alluding to Bannon’s attacks on Romney for his service as a Mormon missionary in France during the Vietnam War. McCain, who more than did his part in Vietnam, made clear he didn’t share Bannon’s view. “I didn’t think there was anything wrong with serving your church. I had no idea that was a crime.”
Two days before Christmas, Larry Fitzgerald, a potential Hall of Fame wide receiver for the Arizona Cardinals, wrote a piece about Senator McCain for Sports Illustrated. Of the Senator, Mr. Fitzgerald said, “One of the reasons I admire Senator McCain is that he doesn’t always just vote his party. He votes his conscience, and that can seem like a rare quality these days.” The article is decent, though not nearly as good as the other ones I’ve referenced. It is further testimony to yet another impressive relationship that Mr. McCain developed.
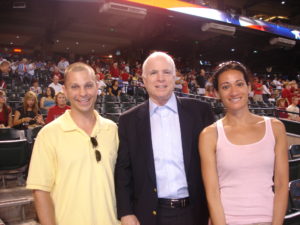
I met Senator John McCain on Memorial Day in 2009. My ex-wife and I traveled to Arizona for the week around my 33rd birthday. We hiked the Grand Canyon (almost to the bottom), biked around Sedona, walked around Flagstaff, took in the Meteor Crater, and attended an Arizona Diamondback game in our quest to visit every MLB park (I’ve done them all and April is more than 3/4 through). Before the game started, I noticed Senator McCain sitting alone. No one had seen him. I felt conflicted. I like to give people their privacy (I sat next to Philip Seymour Hoffman at a steakhouse in NYC once and convinced April to leave him alone, despite the fact that Mr. Hoffman uncannily looked like my longest serving college roommate). Even back in 2009, after having just recently voted against him, I wanted to go over and shake Senator McCain’s hand. I went up to him and told him that I voted for him in the 2000 primary and that I appreciated his service in the Navy and his work in the Senate. I told him that I didn’t agree with him on a lot of issues, but that I had no question about his integrity. He was neither warm nor pleasant, but shook my hand and agreed to pose for the photo that begins this article. After our photo, a bunch of other people realized that someone famous was down behind home plate and they began to line up. I mouthed “sorry” to him but he didn’t respond (he is also known for being difficult and cursing a lot). Before the game, he appeared on the field with his wife and children, one of whom (Jack) was currently serving as a Naval Aviator. Mr. McCain stayed for most of the game and shook hands and signed programs for people that approached him. He never shooed them away.