The Greenagel Equations are a set of practical frameworks developed between 2005 and 2008 in schools, outpatient and family treatment settings. They were built in rooms, not in theory, and have been used with students, families, law enforcement, veterans and therapists.
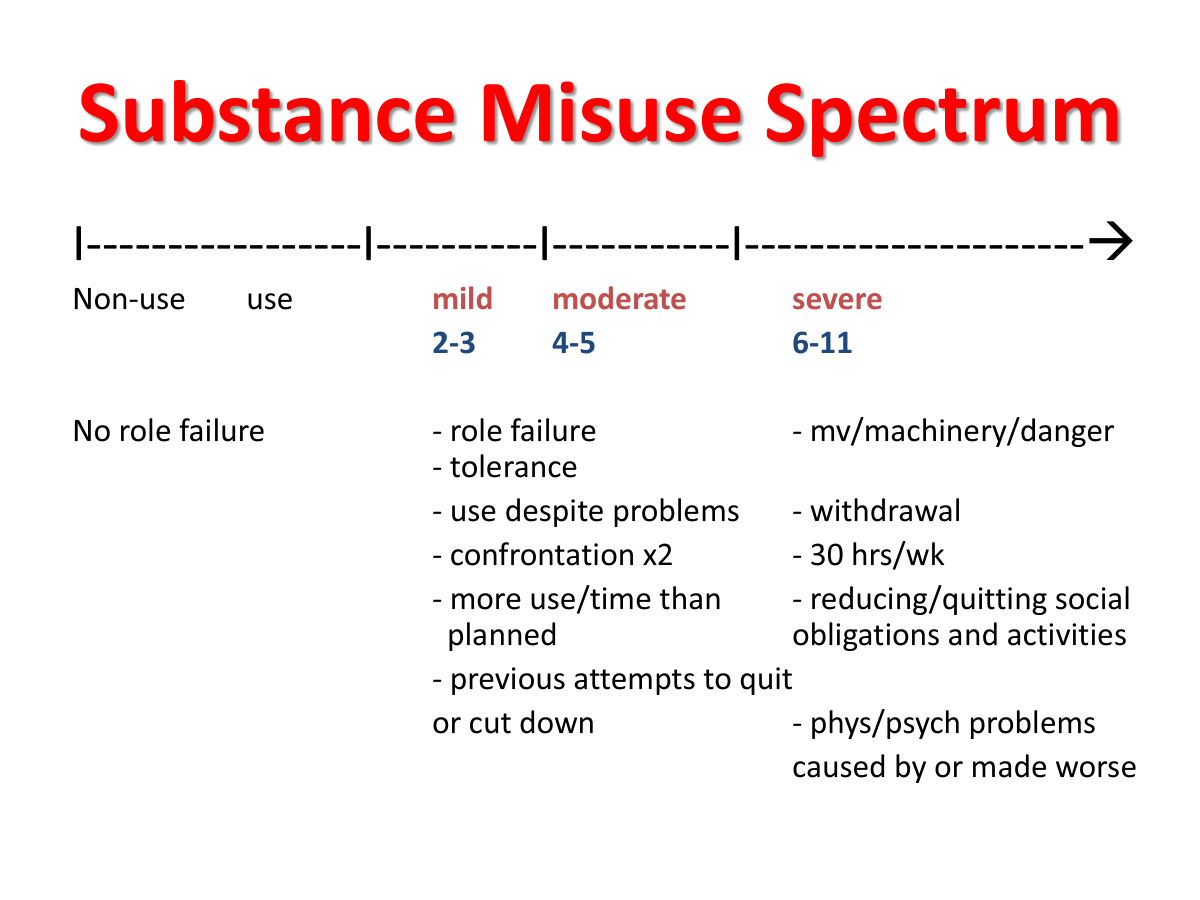
Substance misuse exists on a spectrum from non-use to severe disorder, defined by behavioral, physiological and consequence-based criteria.
I was running a group at Integrity House in 2004 when a client exploded in anger, “I’m tired of all these people telling me I have a problem. You an addict. You an alcoholic. You need treatment. And they keep sending me away to these bitch ass programs.”
“Has anyone ever explained to you how we diagnose someone with substance abuse or dependence?” I asked him.
He immediately calmed down. “No.”
I listed out the criteria from the DSM IV-TR on the board and broke down what each one meant.
Group members started saying what they did and didn’t have. Some confronted each other on their denial. It was a wildly effective group.
I didn’t like how substance abuse had four criteria and substance dependence had seven with only role failure in both. I explained that role failure meant that substance use caused a problem at work, school, with family, with friends, with a romantic partner, legal issues, financial difficulties or health complications.
“All of those?” someone asked.
“No, just one life area needs to be affected.”
I created a spectrum, starting with non-use on the left and then use, abuse and dependence as it moves right. I used role failure as the anchor. Both people who used and those who didn’t use substances were united that they didn’t have any role failure caused by using alcohol or drugs. They may have problems, but they weren’t caused by substances.
For the next nine years, I taught substance misuse as a spectrum, rather than two separate diagnoses. In 2013, DSM-5 came out. It threw out the terms abuse and dependence, got rid of legal problems for diagnosing and listed a clean set of 11 criteria. The APA had come around to seeing this as a continuum, or spectrum. They came to see it my way.
I wanted to include percentages for each group. I looked up data and crosschecked it. For years, it was roughly 20% of adult Americans who do not use alcohol or drugs at all. That about 50-60% use without having any problems and 20-30% meet criteria for a substance misuse disorder. In the 2020s, various data sets place those numbers at 20-30%, 50-60%, and 15-20% respectively.
I have trained and assisted staff and students on the RU Sure Campaign for just about two decades. Their research at Rutgers states that
2 out of 3 students drink 3 drinks or less
and that
1 in 5 don’t drink at all
This breaks down to 20% non-users, which is consistent with my aforementioned data. Whenever I have presented these numbers, especially to people in treatment, correction settings, lawyers, cops or military, I am inevitably met with some version of this comment: “Yo man, your numbers are bullshit.”
People who drink heavily often cannot conceive of that 20% of adults don’t drink at all. “You ever hear the phrase birds of a feather flock together” or “You are identified by the company you keep?”
People nod.
“When I was 15, I was on juvenile probation. My father was horrified. I told him that over half the kids I knew were on probation.”
He responded “juvenile delinquents hang out with other juvenile delinquents. Behavior doesn’t happen in a vacuum.”
Two rules to consider with the spectrum:
- If I take 1000 non-users and 1000 users and then look at them in ten years, there will be more people that meet criteria for a substance misuse diagnosis from the using group than the non-using group. This holds true throughout the spectrum. So, the further along you are, the more likely you are to continue.
- One of the first people I ever treated was a 53-year-old white female who was a middle school music teacher. She met three of the four criteria for substance abuse. She was unhappy, but didn’t have any work or legal or health problems from her drinking. About a month later, I was treating a 15-year-old boy who also met three of the four criteria. He was having problems in school, had been arrested and his parents were both furious and worried about him. His life was already upended and it was very likely that it was going to get worse if he didn’t stop. So, if someone is young and already meets diagnostic criteria, it is much more likely to get worse than someone who is older.
This is the single lesson I have taught more than anything else in my life. I have taught this in high schools, universities, jails, prisons, hospitals, in-patient and out-patient settings, community centers, Army bases, with individual clients and a number of other settings.
Substance misuse exists on a spectrum from non-use to severe disorder, defined by behavioral, physiological and consequence-based criteria.
This is how I explain the criteria in group settings.
Role failure – One challenging aspect is how people define failure. Some students are good with a C, while another student may view a B+ as a total failure. I think it is a good idea for someone to come to a consensus with a counselor on a fair definition of role failure.
Use despite problems – Healthy people cut down or stop when their substance misuse has caused a health, legal, financial or any other type of problem. A doctor tells you to stop drinking and you counter with reducing your drinking for the time being. A counselor tells you that the anti-anxiety medication will be less effective if you use marijuana and you smoke anyway.
Tolerance – It takes more of the substance to get the same effect, or you experience a weaker sensation with the same amount. People will often use a harder version of the substance (80 proof alcohol instead of beer or 74% THC content in a vape instead of 15% THC in the marijuana plant) or combine substances.
Withdrawal – Most people think of shakes and hallucinations when they think of alcohol withdrawal. Those are late stage alcoholism withdrawal features though. More common are headaches, gastrointestinal issues, fatigue and irritability. The most common physical withdrawal feature of marijuana is sleep problems. Psychological withdrawal includes difficulty concentrating, confusion, memory issues, irritability and lack of motivation.
Confrontation (x2) – The DSM-5-TR asks if you have one person in your life who thinks you have a problem. I don’t like that, as there may be someone who has recently quit drinking and wants to change everyone else or is some kind of evangelical teetotaler. I don’t consider unified parents to be two people; I’m also looking for a teacher or coach or friend or romantic partner or the court system to state their concern.
Use of motor vehicle or machinery or other dangerous activities – The number one instinct in all creatures is survival. If you operate a motor vehicle or other machinery while under the influence, you put yourself at increased risk of injury or dying. This goes against nature. Or you get into more dangerous situations than you would when you were not using, you meet the criteria.
Reducing/changing friends and activities – If you used to play softball, sing, paint or ride horses and now you do those things a lot less or not at all, we need to examine whether your use led to this. If you gave up friends that didn’t drink like you or questioned your marijuana use, you probably meet the criteria.
More use, more time than planned – If you bought a 1.75 liter of vodka and planned it to last all of spring break but it ran out on Wednesday, you’re hit. If you acquired 90 Adderall pills for the semester and are out of them by mid-terms, you meet the criteria. If you planned on smoking until 10 pm but you didn’t stop until after midnight, you got it.
Previous attempts to cut down or quit – You once tried to give up marijuana for Lent and you got to day 15 and then said, “Jesus will understand.” You stopped drinking hard liquor and switched to beer, only to eventually get back on hard liquor or drinking an excessive amount of beer. You said only on the weekends and the weekends started on Thursdays. No more bongs, just blunts. This is my last vape. Any of these and you meet the criteria.
30 Hours or more in a week – A week is made up of 168 hours. If you have ever had more than one week (I’ll give you Jamaica 2014) where you were under the influence for 30 hours, you have it. Family members and friends are often aghast at the 30 hours number: “It’s like a full-time job.” Clients I’ve had at group often scoff at the same figure: “I get to 30 hours by Tuesday.”
Physical or psychological problems caused or exacerbated by use – If you got drunk and sprained your ankle. If you had bronchitis and smoked anyway and it lasted for two months. If you never were depressed but now you are down unless you are using, or you had anxiety and you find that since you started smoking, your anxiety has gotten worse.